I recently read Nicole Russell's op-ed piece in USA Today, "The left fueled the male crisis. Now it's shocked."¹ Her argument is that feminism and left-wing cultural messaging sidelined masculinity and then expressed surprise when an entire generation of men started struggling. She cites the suicide rate (four times higher in men) and college completion rates that now favor women. The numbers she uses are accurate. Men are, by most metrics, in trouble in many ways.
It’s hard to disagree with her, but my mind is going in a different direction. She uncovers a cultural villain lurking in the numbers, but I see a healthcare problem.
Per my usual on my many sleepless nights, I was watching YouTube videos, fell down an another rabbit hole, and ended up on the Nightbirde Foundation page. The organization is named for Jane Marczewski, whose singing earned her the golden buzzer on America's Got Talent. But, it wasn't just her voice that got my attention (which means it must have been pretty considerable considering how deaf I've become in recent years). Her heart-breaking message struck me the most. She was diagnosed with cancer at 30 and refused to be defined by it.² She has since passed away and now her name and her mission is carried forward by her foundation through grants and care packages for women with cancer. What caught my eye to most was the title in big, clean white letters across the center of the page:
"No Woman Should Face Cancer Alone."
I looked at that for a long time because there was something that bothered me about it. The concept and the mission is beautiful, but I could not get past the message. Do men not face cancer alone, too? Don't men deserve the same thing? Men are less likely than women to disclose a cancer diagnosis to friends, just as they are less likely to seek emotional support during treatment. They are the ones that disclose much later on, with a more advanced disease, and they die at higher rates from nearly every cancer that affects both sexes.³ Just looking at basic facts, men more often face cancer alone than women do.
The Nightbirde Foundation is doing exactly what it set out to do in a wonderful and effective way. So, that begs the question on where’s the equivalent for men?
Between Russell's op-ed and that late night rabbit hole, the same questions kept popping up in my mind, one political and the other personal. Back in college, I had an English professor who once told our class (to considerable backlash) that each gender is "equal in their misery."
She was describing something I felt but couldn't name. Equal in their misery, but different in the shape of it. The women's health movement built its case around documented clinical failures, including being excluded from research and gaslighted in exam rooms. But what’s not being asked is whether the same tools that found and labeled these issues inside the system could see the same thing for men outside of it.
Russell blamed feminism. I believe the data tells a different story about where the suffering is and who has to infrastructure address it.
I am not writing this as a rebuke to feminism, nor am I defending Nicole Russell's politics. But what I am doing is using data to look at a measurement failure so large that once you see it you cannot understand how everyone missed it.
I hate to say it, but men, not women, are the underserved population in American healthcare, and we’re not in the place to change it.
Start with what you can see before looking at a single bit of data. Every October, NFL players wear pink. The league's audience skews overwhelmingly male, and every Sunday for a month the NFL and others promote breast cancer awareness, which is already the most funded and most visible advocacy in all of oncology. That platform is rarely, if ever, used to tell the men watching to get screened for prostate cancer or colorectal cancer. The men see it, but it’s not a message strictly for them.
In June 2026, Halle Berry came out publicly that her perimenopause symptoms had been dismissed for years, and that her gynecologist once misdiagnosed them as herpes.⁴ Her comparison was pointed in saying that men never have to deal with this kind of treatment. They just get Viagra.
Her dramatic over-generalization of one clinical encounter to a claim about the entire healthcare system is where her framing breaks. Viagra was developed by Pfizer because they wanted to go after a commercial market, not because healthcare prioritized men's health over women’s. The population-level data heads in the opposite direction from her claim. Berry's story is a numerator of one encounter and one patient. I'm arguing for the denominator, which is about who is in the system at all and who the system decided to build for.
Breast cancer awareness dominates oncology fundraising and our collective consciousness by a margins that are difficult to overstate. Movember is the only men's health awareness campaign with any sort of cultural penetration (I might share my photos from that embarrassment if someone pays me), but it can't hold a candle to pink ribbon marketing. Lung cancer kills more men than prostate cancer and gets even fewer campaign dollars. The Nightbirde Foundation is one example of a pattern so consistent it stopped looking like individual choices a long time ago. Cancer support organizations are built on the premise that isolation during illness is something only women face. Men face cancer with fewer organizations trying to reach out to them and with almost no social permission to ask for help.
The mismatch in messaging rests on the institutional disparity’s shoulders and that is what I want to quantify rather than assume.
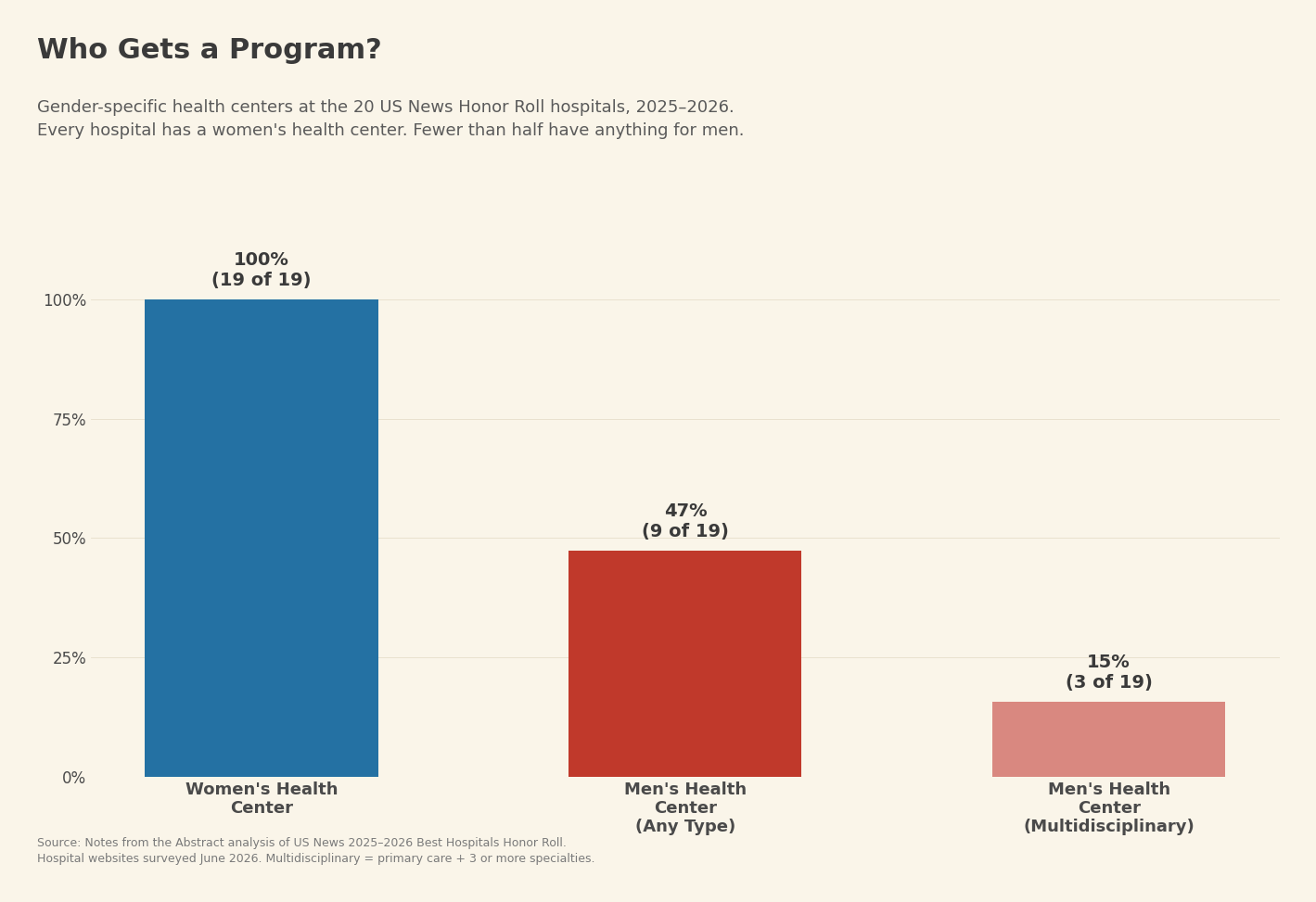
98% percent of the top 50 U.S. hospitals has a women's health center while 32% had any kind of men's health center.⁵ Now, that was measured once, almost a decade ago in 2017. Apparently, it’s not such a pressing issue that no one has cared enough to measure it again since. So I did it myself. I surveyed all 20 US News & World Report Honor Roll hospitals for the 2025-2026 cycle and checked each one for whether they had a branded women's health center and a men's health center.
All hospitals listed on the Honor Roll, 19 of 19 (Mayo Clinic counts once across its two campuses), has a women's health center. 9 of 19, or 47%, have any sort of men's health center. The Honor roll hospitals are the best-funded, most prestigious institutions in the country, and these numbers are the best-case scenario, never mind the disparity at community hospitals and regional systems, which are far worse. Of those 9 men’s centers, only 3 have multidisciplinary programs that offer primary care alongside three or more specialties in a coordinated setting: NYU Langone's Preston Robert Tisch Center for Men's Health, UCLA's Men's Clinic, and New York-Presbyterian's Iris Cantor Men's Health Center.⁶ The remaining 6 are urology departments with expanded branding. Men's health, when it's even covered at all, gets reduced to a prostate and a penis. Women's health programs go well beyond a woman’s reproductive organs to whole-person care—and it’s been that was for decades.
The Iris Cantor Center at New York-Presbyterian opened in the same building as the Women's Health Center that the same donor, Iris Cantor, established in 2002. The men's center came more than twenty years later, funded by a $20 million philanthropic gift. That means, an individual had to write a check to create what the institution built for women on its own.
Those are the best hospitals in the country. Then there's the question of what rural America looks like. Roughly 1,353 Critical Access Hospitals serve rural communities across the United States.⁷ They have 25 beds or fewer and operate on cost-based Medicare reimbursement while constantly fighting to keep their doors open. Case in point, 152 rural hospitals have closed since 2010, including 52 CAHs.⁸ The chance that any of these facilities operates a dedicated men's health program is functionally zero. Justifying an additional department is hard when a hospital is scraping by just to maintain emergency services.
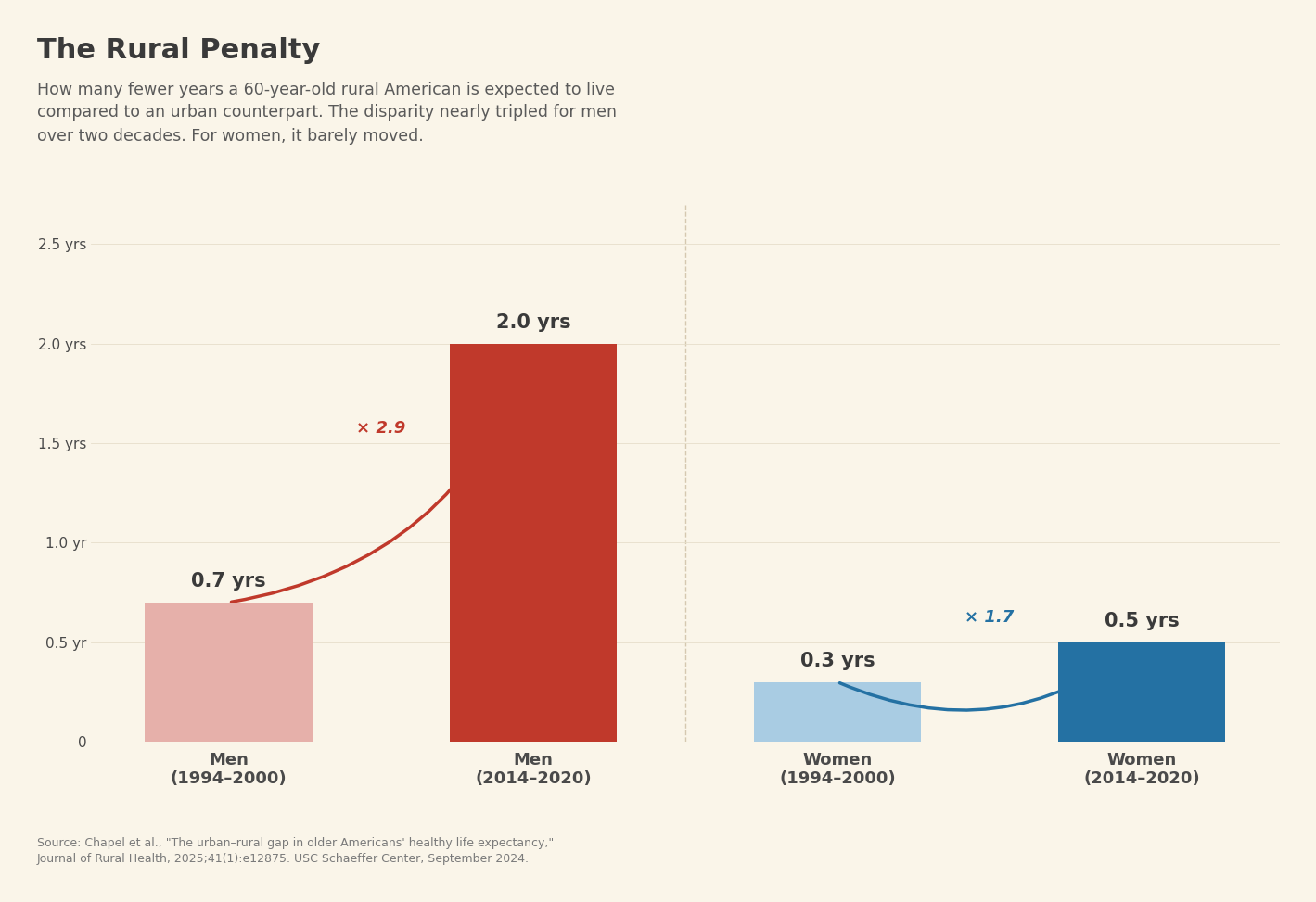
On top of that, the rural health penalty for men has nearly tripled over the past two decades. Sixty-year-old rural men now live two fewer years than urban men.⁹ Rural men also spend 1.8 fewer years in quality health than their urban counterparts. For women, the difference is 6 months. For men, it's two years.⁹
If you’ve read "The Engine and the Fuel," you know Dale Hammond, our intrepid oil field worker in Stamford, Texas, whose fragmented health record I used as a case study in what happens when AI tries to read clinical documentation generated in an under-resourced clinic. Dale is a fictional composite, but the world he lives in is real. The system fails men at the population level and builds almost nothing for them at the institutional level, and in rural America where the need is greatest the resources are thinnest.
Moving from the hospital to the federal government, the differences do not get better. Five Offices of Women's Health operate across the federal bureaucracy: CDC, the FDA, HHS, HRSA, and SAMHSA.¹⁰ The Office on Women's Health at HHS was established in 1991, and in the years since, the federal government has created zero offices of men's health.
NIH spends roughly $700 million annually on breast cancer research and roughly $250 million on prostate cancer, despite comparable mortality between the two.¹¹ Over the decade from 2013 to 2022, breast cancer received $8.36 billion in combined funding compared to $3.61 billion for prostate cancer.¹² Federal cancer research funding correlates well with incidence (r = 0.70) but poorly with mortality (r = 0.36).¹³ Funding likes follow the awareness campaigns, not the body count.
I am not saying there shouldn't be funding for women's health. The Offices of Women's Health increased breast cancer screenings and reduced breast cancer deaths.¹⁰ Those outcomes are the proof of concept the system works. The question is why what works isn’t used for the other.
Now the body count. Male life expectancy in 2024 was 76.5 years. Female life expectancy was 81.4.¹⁴ Men die at an age-adjusted rate of 884.2 per 100,000 compared to 632.8 for women, which is 39.7% higher.¹⁵ The differential widened to 5.8 years in 2021, the largest since 1996, driven by COVID-19 and deaths of despair, both of which hit men harder.¹⁶
I know the counterargument is that men die younger because they smoke more, drink more, and work more dangerous jobs (yes, and do stupid things more—have you seen the TikTok videos lately?). Some of that is true. Men do more dangerous things, and those factors contribute. But do they explain the full picture. After controlling for demographics, behavior, and chronic conditions in a cohort of 47,056 adults, men still had a 63% higher risk of all-cause mortality.¹⁷ Heart disease mortality was 96% higher. Diabetes was 90% higher.¹⁷
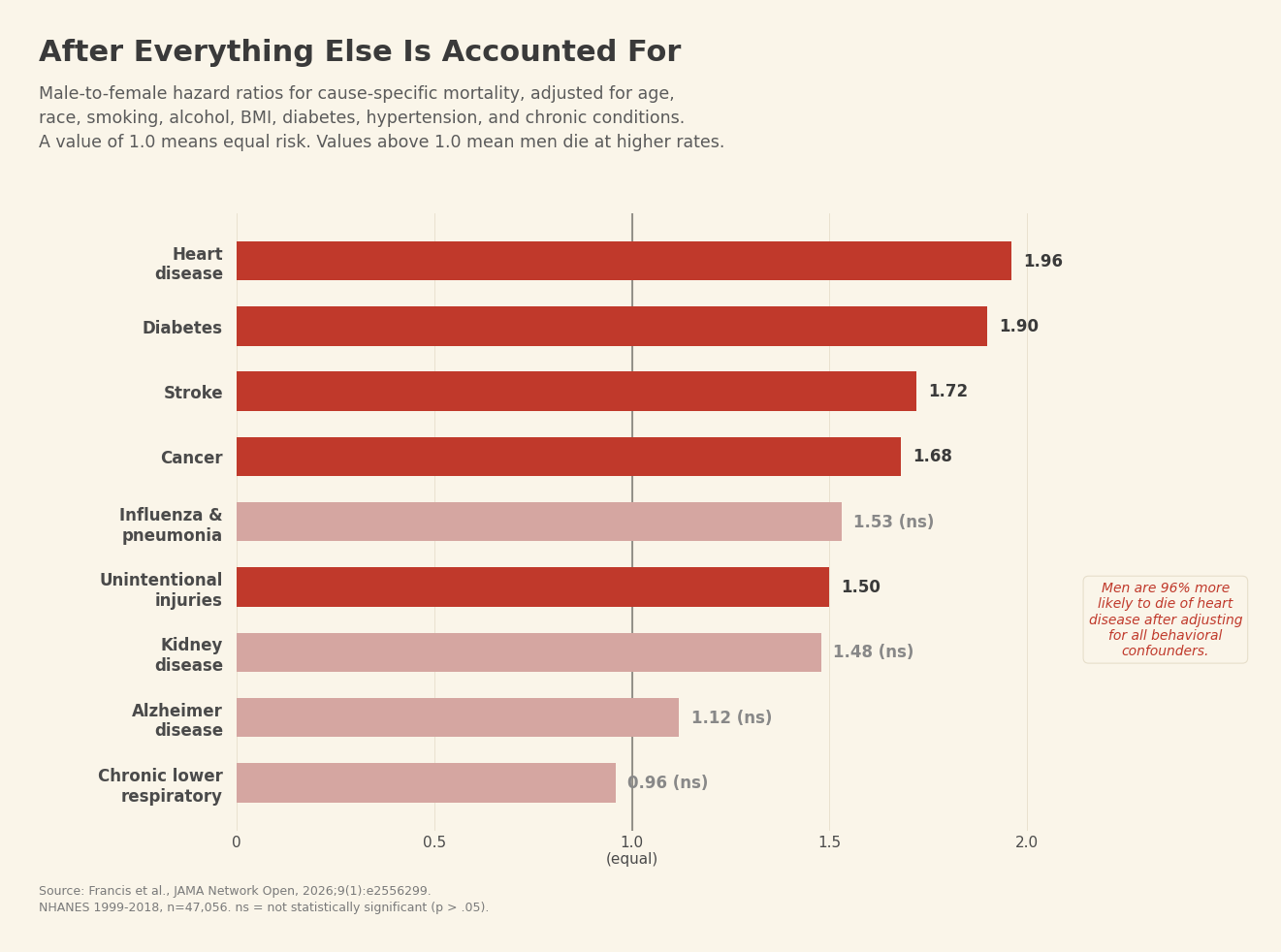
Heart disease and diabetes are conditions the healthcare system is supposed to manage. After removing every behavioral and demographic variable, men still die at dramatically higher rates from both.
Males lost 8.1 million more years of potential life than females in 2023 alone, up 14% since 2000.¹⁸ The excess male mortality rate was narrowing between 2000 and 2014, and then it reversed. After 2014, the trend widened again, concentrated in younger and middle-aged men.¹⁸ The trajectory was slowly improving, and then it stopped.
I want to pause here because these numbers start to blur together after a while, and I think that is a big part of the problem. We are so accustomed to men dying younger that the data doesn’t register as anything unusual, just treated as a feature of being a guy rather than a failure of the system that is supposed to keep people alive.
Let’s get a little darker. In 2024, 48,824 Americans died by suicide. Of those, 38,977 were men, or roughly 80%.¹⁹ That held steady at approximately four to one for decades. Men over 75 have the highest suicide rate of any demographic group in the country.
The counterargument is that women attempt suicide at higher rates, roughly 1.5 to 3 times more frequently, which is absolutely true.²⁰ The research on this strengthens the case. Across 5,212 suicide attempts studied in four European countries, "Serious Suicide Attempts" were rated significantly more frequently in males than females (p < .001), and the finding held even within the same method of attempt.²¹ U.S. data on method lethality are consistent with the European findings.¹⁹ In women, deliberate self-harm more often serves what the literature calls an "appeal function," communicating distress or modifying the behavior of others. In men, it correlates with intent to die.²² Male depression itself presents as what researchers describe as "a distinct clinical phenotype challenging to recognize," meaning it gets missed or undertreated, and by the time suicidal behavior starts manifesting itself, the intent is lethal.²³
Men attempt less frequently and intend to follow through more often, with fewer interventions catching them before they reach the point of crisis.
Dale Hammond is somewhere in these numbers. Not literally (he's fictional, remember), but what he represents is not as 54-year-old man with uncontrolled diabetes with retinopathy diagnosis who sat in his living room one Tuesday night with a severe headache and no place to go. Dale did not choose to disengage from healthcare. There is no men's health center within 200 miles of Stamford, Texas, and no federal office studying why men in his situation die younger than women in the same zip code. The system did not build a door for Dale to walk through, and then it counted his absence as a personal decision.
Now the denominator.
Women go to community health centers at almost double the rate of men, at 445 per 1,000 compared to 249 per 1,000.²⁴ After controlling for age and removing pregnancy-related visits, women are virtually 100% more likely to seek preventive care.²⁵
Women indeed face serious problems inside clinical encounters. Berry's experience of having her perimenopause misdiagnosed is one of thousands of stories. Undertreated cardiac symptoms and delayed autoimmune diagnoses are well-established failures, and the advocacy that grew around them was built in response to what the data told.
Here is where the measurement problem comes in, and where I think the conversation about equity went wrong.
Women have significantly more healthcare encounters per capita than men. More encounters means more opportunities for negative experiences. If a woman sees a doctor four times a year and a man sees one once (or not at all), the woman has four chances to be dismissed or misdiagnosed, and the man has one chance or zero. The raw count of bad clinical experiences will be higher for women even if the per-encounter rate of dismissal is the same between the sexes. Whether anyone adjusted for this is a fair question. The answer is that the equity literature has not asked it.
I am not claiming that women are dismissed at the same rate per visit. The per-encounter data does not exist, and I cannot prove what has not been measured. What I am saying is that the conversation about women's clinical experience was built without adjusting for the most basic epidemiological variable in the room, which is how often each population shows up.
Epidemiologists call this selection bias. When you study only the people who entered the system, your findings describe only the experience of those people. They tell you nothing about the people on the outside. You cannot be gaslit by a doctor you never saw, nor can you have your symptoms dismissed at a clinic you never walked into. The conversation about equity measured the experience of the population that showed up and came to conclusions about who the system is failing. However, those who stayed home were never part of the calculation.
Take the entire population as the denominator rather than the people who sought care, and the picture changes.
The double standard in how public health treats underutilization makes the point on its own. When Black Americans underutilize mental health services, the field identifies structural barriers.²⁷ When men underutilize care at half the rate of women, we call it stubbornness. The barriers are different, but the analytical response should be consistent. Underutilization in one group triggers a systemic investigation; in another, it triggers a character judgment.
The NIH defines health disparities as "largely preventable health differences that adversely affect populations who experience greater challenges to optimal health."²⁸ The populations designated for more attention include racial and ethnic minorities, rural communities, sexual and gender minorities, people with disabilities, and low-SES populations.²⁸ Men are not on that list, despite dying 4.9 years earlier and completing suicide at four times the rate. The designation was designed to identify who is being failed and it counted everyone except the population with the worst mortality outcomes.
Some of the life expectancy difference is biological. Chromosomal and hormonal variation between the sexes is documented, and intrinsic biological factors likely contribute.¹⁷ But that does not survive cross-national comparison without qualification. The life expectancy split between men and women varies from 1.3 years in Bahrain to 10.5 years in Russia.²⁹ If biology were the only driver, the difference would hold constant across societies. Lithuania's extreme male suicide rate followed post-Soviet economic disruption, and the U.S. differential blew open during COVID.³⁰ These are not biological events. Even the biological component, if it is a factor, makes the argument for more investment in men's health, not against it.
Someone might say that men should build their own advocacy movement, the way women did. As a society, we do not tell any other underserved population to build its own infrastructure. The State of Men's Health Act (H.R. 7602) was introduced in 2026 with bipartisan support and backing from the American Urological Association.³¹ The bill uses existing funding and includes explicit guardrails to prevent any money from being diverted from the Office on Women's Health. Despite that, political fear of midterm optics has stalled it. The conversations within HHS about how the office would be structured have gone nowhere because no one wants to stick their neck out.³²
One can't build a men's health movement when the political system is too scared to go after it. This is why I say politics and healthcare should never mix.
Russell asked which cultural force is to blame for men's declining health. The better question is why the same culture built 5 federal offices for women's health and none for men's, and why the top hospitals all constructed women's health programs while only a handful built anything substantial for men.
It’s the culture responsible for masculinity itself. A 2024 WHO analysis found that masculine norms around self-reliance and stoicism are a primary barrier to care-seeking across all ten major disease categories, and that men have "far fewer routine contact points with the healthcare system over their lifetimes than women."³⁴ That thinking predates the women's movement by centuries. Feminism did not tell hospitals to nix men's health centers. Our idea of manhood did, and the people making those institutional decisions (many of them men) could not imagine men as a population that needed to be reached. The men who would benefit most are the ones whose self-concept makes them least likely to demand it be built.
Instead, healthcare constructed women's health programs with forty years of messaging that says, Hey, ladies! Your health matters! Come in! Look! We built this for you!
What's there for men?
The answer is clear, because the women's health movement proved it works. Men's health advocates are hoarse from screaming it: "The Office of Women's Health has done spectacular things for women on so many levels. We've got a template to follow that's been incredibly successful."¹⁰ An Office of Men's Health, built on the same model, could increase screenings and reduce preventable deaths. Adding men to the NIMHD's list of designated disparity populations would force the measurement to account for what it has been ignoring. Screening campaigns in workplaces and veteran organizations would meet men where they are instead of expecting them to find spaces built without them, and the NFL pink campaign has already proved that male-dominated platforms can deliver health messaging at massive scale. That infrastructure has yet to be turned toward the right audience.
HHS found that more than half of elderly women living in poverty were not in poverty before their husbands died.³³ Men dying younger does not only hurt men, but impoverishes their spouses and steals away children's fathers. The women's health succeeded partly by connecting individual health to what it costs a family and a community. Men's health has not made that case, and until it does, the political will to do anything is going to remain stalled in a committee.
My professor was right that each gender carries its own misery. She may not have been right that the scale is equal. Five offices to zero. One hundred percent to 47%. A 63% mortality differential that persists after every behavioral confounder is stripped away.
The data, right now, falls on deaf ears.
References
¹ Russell N. "The left fueled the male crisis. Now it's shocked." USA Today. June 7, 2026.
² The Nightbirde Foundation. nightbirdefoundation.org.
³ BCBSM. "Male Mortality: Why Men Die Earlier Than Women." April 2026; Francis J, Graubard BI, Katki H, Jackson SS. JAMA Netw Open. 2026;9(1):e2556299.
⁴ Berry H. Interview. HuffPost. June 2026.
⁵ Alam R, et al. "The men's health center: disparities in gender specific health services among the top 50 'best hospitals' in America." Int J Mens Comm Soc Health. 2017. PMID: 29264139.
⁶ Original analysis. Notes from the Abstract. June 2026. Dataset and methodology available on GitHub.
⁷ Definitive Healthcare. Critical Access Hospitals in the United States. 2024.
⁸ HRSA Rural Hospital Programs; Sheps Center for Health Services Research. Rural hospital closures since 2010.
⁹ Chapel JM, et al. "The urban-rural gap in older Americans' healthy life expectancy." J Rural Health. 2025 Jan;41(1):e12875.
¹⁰ STAT News. "Women's health has federal offices. Should men have one, too?" March 12, 2026; GM Today. "Why we need an office of men's health — now!" October 2021; AFRO American Newspapers. November 2021.
¹¹ "Why Prostate Cancer Research Funding Is so Low." Fatherly. October 2021.
¹² Nuzzo JL. "Prostate and breast cancer funding." The Nuzzo Letter.
¹³ Kamath SD, et al. "Disparities in NIH and federal cancer research funding across different cancer types." J Clin Oncol. 2025;43(16_suppl):11025. ASCO 2025.
¹⁴ CDC/NCHS Data Brief No. 548. "Mortality in the United States, 2024." January 2026.
¹⁵ MMWR. "Mortality in the United States — Provisional Data, 2023." August 2024; CDC/NCHS Data Brief No. 521. December 2024.
¹⁶ Harvard T.H. Chan School of Public Health. "U.S. men die nearly six years before women, as life expectancy gap widens." November 2024.
¹⁷ Francis J, Graubard BI, Katki H, Jackson SS. "Sex and All-Cause Mortality in the US, 1999 to 2018." JAMA Netw Open. 2026;9(1):e2556299.
¹⁸ [VERIFY BEFORE PUBLICATION — American Journal of Medicine, April 2026. Search: "sex differences all-cause cause-specific mortality years of life lost United States 2000-2023." PMC may have it indexed under PMC12859720.]
¹⁹ AFSP. "Suicide Statistics." 2024 data. Retrieved April 2026.
²⁰ CAMS-CARE. "Gender Paradox in Suicide: Men, Women & TGD Differences." March 2026.
²¹ Cully et al. "The gender paradox in suicidal behavior and its impact on the suicidal process." ScienceDirect. 2011. EU-funded OSPI-Europe project, n=5,212.
²² Ibid.
²³ "The gender paradox in suicide: Some explanations and much uncertainty." Chapter, Springer. 2021.
²⁴ Axios. "Big gender gap seen in health center visits." October 22, 2024; CDC/NCHS National Health Statistics Reports No. 211. October 2024.
²⁵ CDC/NCHS Data Brief No. 234. "Preventive Care Visits, 2012." January 2016.
²⁶ INTEGRIS Health / CDC. "Why Don't Men See Doctors?" June 2019.
²⁷ NIH/NIMHD. Health disparities frameworks and designated populations.
²⁸ NIMHD. "NIH-Designated Populations with Health Disparities."
²⁹ Rochelle TL, et al. "The male disadvantage in life expectancy: can we close the gender gap?" PMC (PMC7928849).
³⁰ "Gender equality and the gender gap in life expectancy in the EU." PMC (PMC8845192); FREE Network. "Gender Gap in Life Expectancy and Its Socio-Economic Implications." 2024.
³¹ "Bill Proposed for US Office of Men's Health." Psychiatry Advisor. June 2026; AUA press release on State of Men's Health Act (H.R. 7602).
³² "A federal office of men's health has never been closer, yet it's likely still years away." STAT News. May 22, 2026.
³³ STAT News. March 12, 2026.
³⁴ Davis S, Ameyan W, Medley A, Toledo C. "Mobile Wellness in the Workplace: Addressing the Global Men's Healthcare Gap, from a WHO Framework Perspective." PMC (PMC11652426). December 2024.